Why
pediatric MS important
-
Treating kids is always important
-
Many missed opportunities because diagnosis
is delayed, yet early treatment is critical
-
Studying pediatric MS may increase our
understanding of the pathogenesis of the disease and help all patients with
MS
Unique
Challenges
•
The diagnosis of
pediatric MS is increasingly being considered
-
Wide spread availability of MRI
-
Need for early diagnosis & treatment
•
Demyelination in
the presence of ongoing myelination within the brain raises unique issues
•
Rapid diagnosis
and treatment is limited by lack of clinical experience
Epidemiology
•
2.5 million
people affected world-wide
•
3.5-5%
symptoms before 18 years
–
(100,000-200,000
world-wide)
•
0.2-0.7% onset
before 10 years of age
•
MS as young as 2
years is reported but uncommon
Gender
Distribution
|
Age
|
Female: Male
|
Ref
|
|
< 10 years
|
0.6: 1
|
Simone 2002
|
|
10 – 14 years
|
2.6:1
|
Simone 2002
|
|
13 years
|
3.5:1
|
Boiko 2002
|
|
14 years
|
7.5:1
|
Boiko 2002
|
Definitions
•
Acute
Disseminated Encephalomyelitis
(ADEM)
•
Clinical
Isolated Syndrome (CIS)
•
Neuromyelitis
Optica (Devic Syndrome)
•
Pediatric
Multiple Sclerosis
(Pediatric MS)
ADEM
•
Acute
Demyelinating CNS Disorder
•
Usually a one
time event
•
Typically
Affects Children
•
Monophasic
Course
•
Focal or
Multi-focal Neurologic S&S
•
Multi-focal
Demyelinating Lesions (MRI),
grey and white matter
•
Behavioral/ or
Mental Status Changes
•
Seizure
•
Prodromal
Illness (≥70 %)
•
Fever, Headache,
Nausea/Vomiting/
¯
Appetite, Lethargy
ADEM
Clinical Characteristics
Signs &
Symptoms evolve over time
Maximal deficits reached ~ 1-2 weeks
Resolution
rapid
/ or weeks to months
may
/ may not be complete
Repeat MRI
®
resolution / no new lesions
ADEM:
Laboratory Findings
CSF
mild pleocytosis(↑wbc)
+ ↑ protein
+ OCB (Oligoclonal Bands) / IgG
production
(uncommon -
transient)
MRI
white matter and grey matter lesions
(bilateral, asymmetric)
Usually spare periventricular areas
+ Basal ganglia involved
lesions highly variable size and number
punctate - large & confluent -
tumor-like
Usually resolve
ADEM
At onset
8 wk
f/u
FLAIR MRI
ADEM
Differential Diagnosis
INFECTIOUS
ILLNESSES
-
Measles -20-30% deaths
-
Influenza A or B
-
Hepatitis A or B,
-
Coxsackie virus
-
Vaccinia
-
winter/spring
respiratory viruses
-
Herpes virus
infections
-
(HSV,VZV, HHV6, CMV,
EBV)
IMMUNIZATIONS / VACCINATIONS
Rabies
Diptheria -Tetnus-Pertussis
Hepatitis B
Smallpox
Vaccines now devoid of neural elements
Successful immunization programs,
virtual eradication of
small pox disease
ADEM
Evaluation
|
–
CSF
–
Lactate-Pyruvate
–
Cytology
–
IgG
Index; OCB
–
R/O
CNS infection
CSF profile, CSF viral & bacterial cultures
PCR-
especially for Herpes Simplex Virus
Lyme
titer
Measles Ab
|
Blood
CBC/diff, Electrolytes, LFTs, ESR
T4/TSH, B12, Biotinase
ANA, Anticardiolipin Ab, Antiphospholipid Ab,
ACE
Lupus Anticoagulant
VDRL/RPR
CADASIL, LHON mutation
Mitochondrial gene mutation
Lactate-Pyruvate
|
ADEM
treatment
-
Corticosteroids
-
Supportive Care
-
Symptomatic Treatment
-
Therapy targeted to
immune-mediated process
-
Currently, no
treatment trials or proven protocols for ADEM
ADEM-
the dilemma
myriad of terms found in the literature
biphasic
multiphasic
relapsing
recurrent
steroid dependent
Neuromyelitis Optica
(Devic’s)
Disease
Courses in MS: Types of MS

Unusual
Demographic Pattern
Frequency of Pediatric MS
Why are
kids different?
Differences between Adults and Children with MS
-
Less common
-
More often RR onset
-
Overlap in clinical
presentation
-
Response to disease
modifying therapy
-
Conversion to SP
somewhat slower (?)
-
Very severe subset (?)
-
Demographic pattern
may differ?
Differences between Adults and Children with MS
-
Average time to
recovery shorter
-
Lower overall
disability after attack
-
Higher relapse rate
-
Shorter time between
first and second attack
-
Kids may be more
likely to have seizures
Pediatric MS Differential Diagnosis
Supporting laboratory findings-CSF for MS
Clinical
Features
-
Relapsing remitting
onset usual course
-
Systemic sx
occasionally
-
Onset may be with
sensory, gait, visual or balance problems
-
Cognitive problems may
be present (33%)
-
OCB usually positive
-
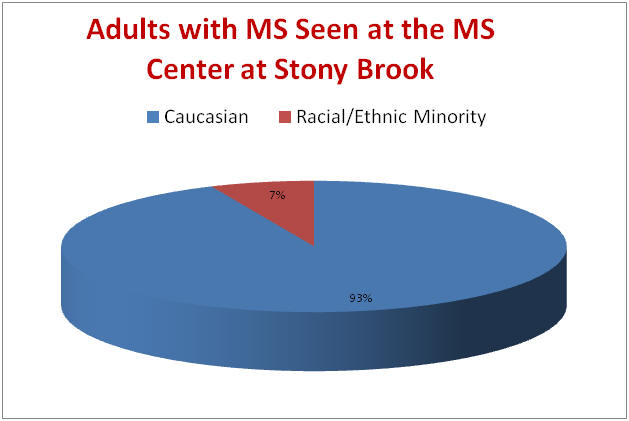
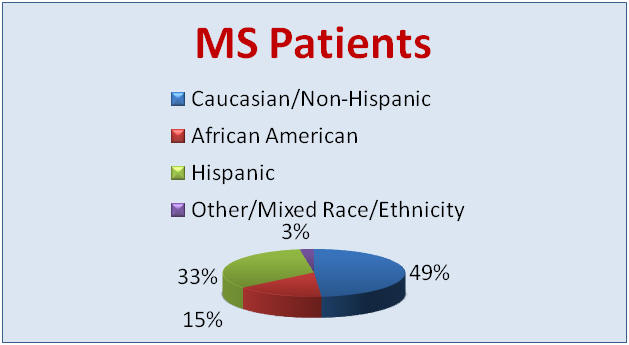
In some regions of the
USA: high number of minorities affected
How do
these kids present?
-
Optic Neuritis
-
Sensory changes
-
Motor disturbance
-
Ataxia/balance
Presentations in Ped MS
Banwell,
Neurology in press
Criteria for Pediatric MS
“McDonald” MRI criteria: TIME
-
1st scan < 3 months
after clinical event, then repeat 2nd scan 3 months from event
-
if above not met,
repeat scan 3 more mos.
Clinical Management
-
Treatment must involve
entire family
-
Education, reassurance
-
Medication for symptom
management
-
Urinary
dysfunction
-
Spasticity
-
Depression
-
Disease modifying
therapy should be given
Experience with Disease Modifying Therapies
-
All DMT medications
are well tolerated
-
Side effects similar
to that of adults
-
In (< 10 years) on
IFN, monitor LFTs at onset
-
Clinical impression is
that DMT helps reduce relapses and MRI progression
-
No data on “best” drug
for kids
Experience with DMT
Experience with Disease Modifying Therapy
Chemotherapy in Pediatric MS
-
Novantrone
-
Cytoxan
-
Imuran
-
Rituxumab (Rituxan)
-
Natalizumab (Tysabri)
Management of Relapses
Symptomatic Management
-
Attention
-
Fatigue
-
Memory
-
Pain:
-
Anticonvulsants,
antispasticity agents, anti-inflammatory, physical therapy, exercise
-
Depression
-
Spasticity
-
Bladder dysfunction
-
Nutrition
-
Rest
-
Plan activities
-
Heat
-
School modifications
Special needs for families with child with MS
-
Ped MS patient is
isolated
-
Families are
frightened
-
Current support
mechanisms are limited
-
Special issues relate
to school and social interactions
Psychosocial problems
Causes of Psychosocial Problems
-
Issues specific to MS
-
Rare in children
-
Physical symptoms
(vision,motor, bladder)
-
Uncertainty of the
disease course
-
Uncertainty of
treatment effect
-
Unpleasant
treatment modalities
-
Injection
phobia
-
Medication
side effects
Consequences
-
On the family
-
On the school
experience
Role of health care provider
-
Encourage open
communication
-
Involve family and
child with decision making process
-
Medication choices to
fit child’s lifestyle
-
Continuously
re-evaluate goals and plans
-
Provide reassurance
-
Be available to
child
-
Family
-
Emphasize there are
others affected, “you are not alone”
Weekend Retreat